{kind=link}
20 years of the Estonian Constitution
XIX/2012
ISBN 978-9985-870-29-7
Issue
Mortality Rate and Causes of Death of Delinquent Individuals: Data from the Estonian Longitudinal Study of Criminal Careers
1. Introduction
This paper focuses on the risk of early death and dying of natural and unnatural (external) causes among former juvenile delinquents in Estonia. We examine first the question of to what extent former juvenile delinquents have a greater risk of dying earlier and dying of different causes than the general population in Estonia do. Secondly, the paper looks at the differences in mortality rates and causes of death between persistent and desisting offenders. Thirdly, we compare mortality rates for cohort members and causes of death among Estonian and non-Estonian delinquents.
2. Delinquency and mortality
It is a well-established empirical fact that delinquent individuals have higher death rates than do non-delinquent individuals. In a longitudinal study of juvenile delinquency and adult crime up to age 32, the Gluecks found that the death rate for delinquents was twice that of matched non-delinquent individuals. *2 Laub and Vaillant used the Gluecks’ original data and followed almost 500 delinquent and 500 matched non-delinquent comparison males until age 65. According to their findings, delinquent subjects were more than twice as likely to die (51%) as the 196 boys with no unofficial delinquency (23%) from natural or unnatural causes. *3 In a 30-year follow-up, Robins and O’Neal found a mortality rate for problem children with conduct disorder by age 40 that was twice as high as that of control-group members. *4 Other longitudinal and follow-up studies that have followed delinquent boys into adulthood have observed similar trends. Rydelius, in following 832 Swedish boys, inmates of probationary schools, noted a death rate by age 40 that was four times higher than statistically expected. *5 In a study of an unselected birth cohort of 12,058 children born live in Northern Finland in 1966, Räsänen and colleagues found that by their 27th birthday the mortality rate of men with combined personality disorders and criminality was more that three times higher than the average for the age cohort. *6
Lattimore and colleagues examined the risk of death among young male serious offenders who were paroled from the California Youth Authority and followed for 11 years. Among 1,998 subjects, they found, 109 (5.5%) had died, for twice the expected rate. *7 Nieuwbeerta and Piquero found in their study that in the subsequent 25-year period in the Netherlands, convicted criminals run about 1.8 times as much risk of dying as the average citizen. The risk of dying of natural causes was 1.6 times as high, and the change of dying of unnatural causes was 2.5 times as high. *8 Another seven-year follow-up study, of 118 formerly incarcerated delinquents, revealed an extremely high mortality rate for the sample. Seven individuals (5.9%) among those studied died before their 25th birthday, putting them at 58 times the national average for individuals in their age group. *9 A study by Teplin et al. revealed the overall mortality rate among delinquents to be more than four times the general-population rate. *10
Criminological theories and developmental or life-course theories anticipate a difference between life trajectories among offenders (desisting, persistent, etc.). Following these theories, one can hypothesise that serious offenders have a greater risk of premature and unnatural death when compared to non-offenders or sporadic offenders. However, as Nieuwbeerta and Piquero *11 note, surprisingly few studies have concentrated on exploration of the relationships among criminal careers, mortality rates, and causes of death. There are two very popular general perspectives that offer explanations as to why delinquent individuals might have a higher death rate. According to the first perspective, criminals die earlier and experience more premature deaths as a direct consequence of their delinquency and way of life. The same individual trait—a low level of self-control—accounts for the relationship of antisocial behaviour with premature death. *12 Gottfredson and Hirschi have argued that human behaviour is consistent across various situations. Individuals with low self-control have a high probability of succumbing to the temptations of short-term pleasures with little regard for the long-term negative consequences.
Indeed, it is relatively well known that, among other things, offenders engage in more risky sexual behaviour, are more often victims of violent crime, and are more involved in accidents of various types than non-offenders. *13 Standing out with a special role in the elevated mortality among delinquents is substance abuse. Offenders tend to die earlier because they engage more often in excessive alcohol and drug use, which increase the risk of premature death. Excessive drinking has a number of harmful effects. It increases the risk of cancer of the liver, stroke, cerebral infarcts, and damage to the coronary arteries. *14 Research has found that offenders are more frequently involved in traffic accidents. *15 Studies have also found that involvement in crime was associated with more than double the likelihood of involvement in risky behaviour in traffic. *16 One of the strongest correlates of crime is the linkage between offending and victimisation, as offenders themselves are at a high risk of being victimised. *17 Lattimore and colleagues found in their study that 47% of premature deaths of paroled offenders were a result of homicide. *18 In the prospective study of the Northern Finland 1966 birth cohort, it was found that, for those individuals who had died by age 27, all deaths were of external causes and 95.5% of deaths were homicides or legal interventions. *19 There is evidence of a link between adolescent and youth suicides and delinquency. *20
Summarising the research on mortality rates and causes of death, one can conclude that offenders are more likely to die in their early years and are more likely to die from unnatural causes (i.e., accident, homicide, or suicide) and natural causes (i.e., diseases). The lower self‑control rate is related to a higher probability of delinquency and high-risk behaviour that, in turn, can lead to premature death. Accordingly, the mortality rates of serious offenders should be higher than those among sporadic delinquents or non‑delinquents for both unnatural and natural causes. From these findings, we can hypothesise that involvement in criminality can predict risk of death; e.g., the longer and more serious the criminal involvement is, the higher is the risk of premature death.
The second perspective is based more on the fact that low socio-economic status and general deprivation lead individuals to poor education and low job status, which, in turn, lead to (chronic) illness and premature mortality. *21 Lack of self-care due to a dysfunctional upbringing, parental neglect, and social deprivation can result in increased and early mortality. Adolescents from dysfunctional families often have problems at school, are truant, and consume drugs or alcohol. Delinquency in such cases is a result of socio-economic deprivation. Offenders of this sort, who actually need social support, became subjects of social control and are sent to special institutions for juveniles.
The last perspective has received less attention and empirical support in the international literature. However, it seems to be important to discuss in the context of the large-scale socio-economic changes that Estonia has experienced over the last 20 years. The challenges of transition were especially great for the non-Estonian population. The study examining ethnic differences in mortality rates in Estonia has shown that in 1989–2000, ethnic differences in life expectancy increased from 0.4 years to 6.1 years among men and from 0.6 to 3.5 years among women. In 2000, Russians had higher mortality than Estonians in all age groups and for almost all causes of death selected for study. The authors conclude that political and economic upheaval, increasing poverty, and alcohol consumption can be considered the main underlying causes of the widening ethnic mortality gap. *22 Taking this into account, our next hypothesis is that we can expect higher mortality rates for non-Estonian delinquents as compared to Estonians in our sample.
3. Method
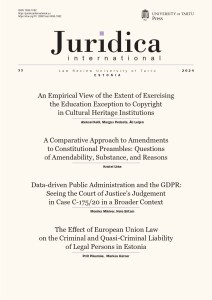
The Estonian Longitudinal Study of Criminal Careers (ELSCC) commenced in 1983. The initial sample of 317 delinquents aged 14–17 constituted the total population (the cohort) of male inmates at two special institutions for juveniles in Estonia. In the first wave of the study, all respondents were interviewed and data from personal files characterising their family background, path of education, and deviant behaviour were gathered and analysed. Three later waves (in 1990, 1995, and 1999) of the study were conducted without direct contact with respondents. Official data from criminal registers, the census bureau, and mortality statistics were collected. *23
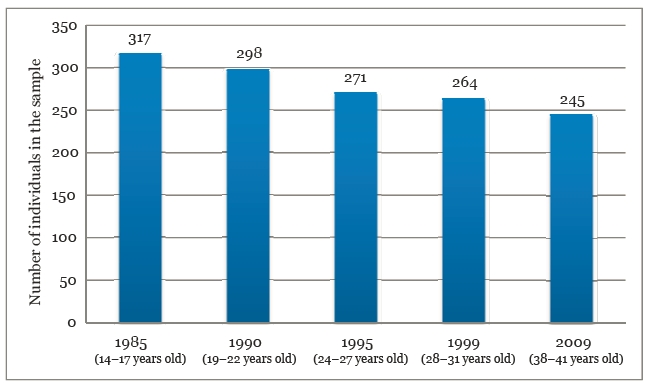
Figure 1. Five waves of data collection—age and number of individuals remaining in the sample.
The fifth wave of the ELSCC work started in 2009; the main aim was to develop a comprehensive picture of persistence of and desisting from criminal activity in middle age. An updated enquiry was dispatched to the Census Registry for all individuals in the sample. The data were obtained in April 2010, with the following information: whether or not the person was featured in the database, status (alive/dead), date of death, country of residence, and residential address (in cases of a foreign country, the state and date of departure). In all, there were 245 individuals in the sample in 2009, 229 individuals were still alive and living in Estonia, 48 had died, and there was no information about 24 individuals in the registers. The data on crimes and convictions over the past 10 years were obtained from penitentiary and criminal registers.
From the Estonian Causes of Death Registry, information was obtained for the date of death and the cause of death of the individual, following the International Classification of Causes of Death (ICD-10). Cause-of-death data were unavailable for three people; in all of these cases, the person had died abroad.
For evaluation of the mortality of sampled individuals, statistical analysis of data was conducted by the Department of Epidemiology and Biostatistics at the Estonian National Institute for Health Development. The cohort was linkedwith the Estonian Causes of Death Registry for gaining of information on date and cause of death in 1985–2009. Each member of the cohort contributed person-years from 1 January 1985 until the date of death, the date of emigration, or 31 December 2009, whichever was earliest. Then we calculated the standardised mortality ratio (SMR) and its 95% confidence interval (CI) for all causes of death, with external causes of death examined separately. *24
The SMR compares the mortality experience of the cohort with that of the general male population of Estonia. The SMR is the ratio of deaths observed to deaths expected. The number of deaths observed and person-years in the cohort were calculated, by five-year age groups, separately for five calendar periods (1985–1989, 1990–1994, 1995–1999, 2000–2004, 2005–2009). The expected number of deaths was calculated by multiplying the number of person-years for the cohort by the appropriate mortality rate for the general male population on the basis of calendar periods and age groups.
An important question would be to what extent some groups of former juvenile delinquents with distinct offending trajectories (for example, persistent v. desisting offenders) run greater or smaller risks of dying of various causes.
Individuals in the sample are compared across two groups differentiated on the basis of offending trajectories up to 30 years of age. The first group is composed of individuals for whom a special institution remained the only punishment recourse. This group comprised 104 individuals (33.1%), who are called sporadic offenders below. The second group consists of individuals who were punished for committing offences at least twice. This group of 210 individuals (66.9%) in the further analysis is called ‘persisters’. *25
Of all delinquents in the initial cohort, 60.5% were Estonians (n = 191) and 39.5% of other nationalities (n = 126). Among the non-Estonians, the main group were Russians (n = 110) and 16 individuals were of other nationality (Ukrainians, Finns, Belarusians, and Armenians). Because all non-Estonian nationals were Russian-speakers, they were analysed as one group distinct from Estonians.
4. Results and discussion
The majority of causes of death (nearly 70%) was attributed to external circumstances, predominantly of a violent nature. Ranking first were homicide and suicide, accounting for, respectively, 17% and 13% of all cases. Alcohol poisoning and death in traffic accidents were each represented by three cases. Of all deaths from disease (non-violent deaths—nearly 30%), the absolute majority were accounted for by diseases related to way of life (cirrhosis of the liver, heart failure, tuberculosis, and epilepsy). The non‑violent deaths too were often related to an unhealthy way of life and alcohol abuse.
Table 1: Causes of observed deaths in the former-juvenile-delinquent cohort in Estonia, 1985–2009
Cause of death | International Classification of Diseases (version 10 codes | No. of cases | Percentage |
Diseases of the circulatory system | I21, I42, D50 | 3 | 6.2 |
Diseases of the respiratory system | A15, A16, A19 | 3 | 6.2 |
Diseases of the digestive system | K70 | 3 | 6.2 |
Other non-violent causes | G40, W13, W78, W79 | 4 | 8.3 |
All natural causes |
| 13 | 27.1 |
Assault or homicide | X93, X99, Y04 | 8 | 16.7 |
Self-injury or suicide | X60, X70, X78 | 6 | 12.5 |
Accidental poisoning by alcohol | X42, X45 | 3 | 6.2 |
Traffic accident | V03, V09 | 3 | 6.2 |
Undetermined and other external causes | R99, X31, X59, Y35 | 12 | 20.8 |
All external, unnatural causes |
| 32 | 66.7 |
Unknown causes |
| 3 | 6.2 |
All causes |
| 48 | 100.0 |
During follow-up of 6,889 person-years, there were 40 persons who had left the country or who were lost for follow-up purposes. By 31 December 2009, 229 people in the sample were alive. We observed 48 deaths in the cohort while the expected number was 22.5. Therefore, the SMR was 2.13 (95% CI: 1.57–2.83) for all causes of death, showing that mortality in the cohort was significantly higher than that of the general male population of Estonia. Also, the members of the cohort had a 109% greater significant risk of death of external causes (32 deaths observed, 15.4 expected; SMR =2.09, 95% CI: 1.42–2.96) than the reference population did.
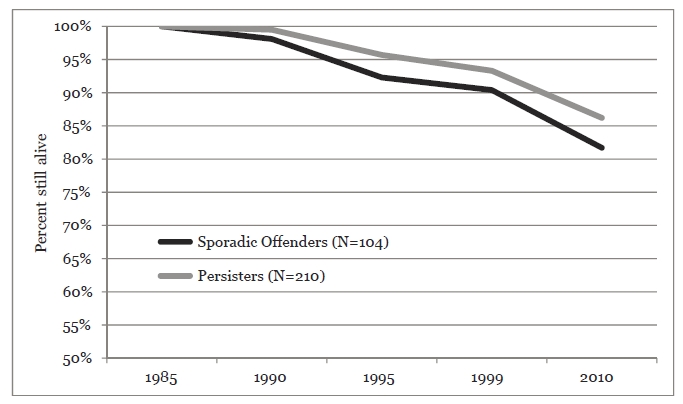
Figure 2. Survival rates for the two trajectory groups.
Looking at survival rates for sporadic offenders and persisters, we can see a somewhat higher survival rate for persisters and a lower one for sporadic offenders. By 2010, approximately 82% of sporadic offenders were still alive, while the equivalent figure for persisters was 87%. The difference between the groups is not statistically significant. Thus, the results have not confirmed the hypothesis of a higher survival rate among sporadic offenders. Furthermore, as the graph shows, they tend to have a lower survival rate than persisters do. There were more suicides committed and a higher percentage of death of natural causes among sporadic offenders. In general, persisters have had a higher risk of death from unnatural and external causes when compared to sporadic offenders.
Table 2: Risk of death due to various causes for the two trajectory groups
Cause of death | Risk of dying | |||
Sporadic | Persistent | |||
n | % | N | % | |
Natural causes of death | 4 | 21.1 | 5 | 17.2 |
Unnatural causes of death | 11 | 57.9 | 18 | 62.0 |
– murder and assault | 3 | 15.8 | 5 | 17.2 |
– suicide | 3 | 15.8 | 3 | 10.3 |
– other unnatural external causes | 5 | 26.3 | 10 | 34.5 |
Unknown causes | 4 | 21.1 | 6 | 20.7 |
Total deaths | 19 | 100 | 29 | 100 |
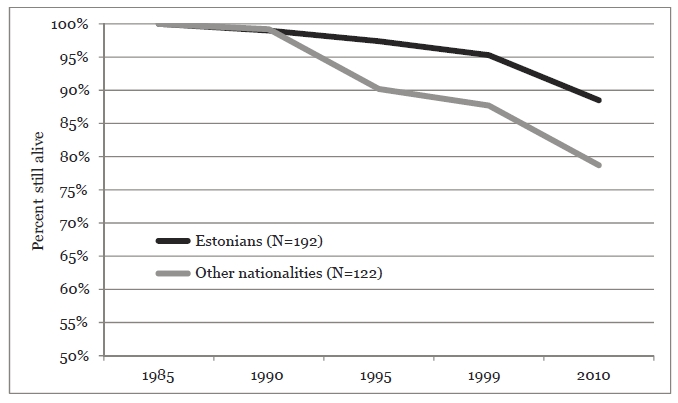
Figure 3. Survival rates among Estonian and non-Estonian delinquents.
The comparison between Estonians and non-Estonians indicated statistically significant differences (p < 0.05) between survival rates for the years 1995, 1999, and 2010. While 88% of Estonian delinquents in the cohort were still alive in 2010, the survival rate for the non-Estonian population was 78%. This result supports the hypothesis of a higher mortality rate for non-Estonian delinquents. The risk of death of natural causes was higher for Estonians, while non-Estonians had a greater risk of death from external and unnatural causes. Estonians had a somewhat higher rate of death through murder and assault and by suicide. Non-Estonians had a higher risk of death from other external causes. This category includes, among others, such causes of death as alcohol poisoning and freezing to death.
Table 3: Risk of death of various causes for Estonian and non-Estonian delinquents
| Risk of dying | |||
Cause of death | Estonians | Non-Estonians | ||
| N | % | n | % |
Natural causes of death | 5 | 22.7 | 4 | 15.4 |
Unnatural causes of death | 12 | 54.5 | 17 | 65.4 |
– murder and assault | 4 | 18.2 | 4 | 15.4 |
– suicide | 3 | 13.6 | 3 | 11.5 |
– other unnatural external causes | 5 | 22.7 | 10 | 38.5 |
Unknown causes | 5 | 22.7 | 5 | 19.2 |
Total deaths | 22 | 100 | 26 | 100 |
There are different and in some ways controversial positions with regard to the connection of morbidity and mortality of criminals. The way of life constituted by having a criminal career seems in general not to be good for an individual’s health. On the one hand, an active criminal career is predictive of a higher mortality and morbidity rate in comparison to the non-delinquent population. However, if one examines causes of death in more detail, different circumstances related to mortality emerge. For example, favourable effects on inmates’ health of serving the term in custody have sometimes been found. In prison, everybody is subject to a healthy daily routine and constant medical observation. This results in a better standard of physical health among inmates than with individuals of the same social status in the population at large. Incarceration may actually serve as a protective factor, as a shield for offenders, precluding an early natural death. Furthermore, research in the USA and France has found that rates of mortality from natural causes are lower for prisoners than in the general population. *26
The setting of standards for prison conditions is characteristic of Western democratic societies. The situation of Estonian prisons relative to that in those Western countries continues to be fundamentally different. Prison inmates in Estonia still have very high HIV and TBC rates. The analysis of causes of death (especially for the time until the mid‑1990s) for individuals in the cohort of this study also characterises prison as an unfavourable environment. These data show that observed homicides (three cases) and suicides (three cases) among individuals in the sample population have been committed in substantial numbers in prisons.
Prison has a dual mortality-risk-reducing effect: in addition to a more organised and healthy lifestyle, a normally functioning prison protects inmates from violence. It was seen in Estonian data too that the health care that a delinquent receives in prison is better than that outside its walls. In Estonia, there is one more specific circumstance related to prisons. As prisons are considerably improved to meet European standards, there is a growing gap between living conditions and services available in prison, on one hand, and offenders’ usual living conditions, in favour of prisons. In Estonia, prisons became a substitute for social-welfare institutions. This thesis is supported by the differences in mortality rates between Estonian and non-Estonian delinquents. The mortality risks for non-Estonians probably accumulate, with this being reflected in the higher mortality rates among them.
5. Conclusions
In summary, the Estonian survey data supported the premise of high mortality of criminals as compared to non-criminals. The indicators of mortality of former juvenile delinquents as measured by the SMR method are, for both general mortality and violent deaths, very high and significantly exceed the corresponding indicator values for the general population. Similarly to the research results in other countries, the mortality rate seen among individuals in the cohort was more than twice as high as that of the general population.
The Estonian situation is noteworthy for specific, dramatic social-economic changes having taken place since the early 1990s. A significant difference between mortality rates was found by nationality: non-Estonian delinquents had higher mortality rates than Estonians did. These results characterise the situation in Estonia, where non-Estonian delinquents experience more risks and are marginalised more often than are Estonians.
Studies of mortality of criminals had until now been carried out exclusively in the developed Western countries, and in other countries diverse circumstances may emerge. The important aspect of the study described here lies in its social-political context. The results presented here lead to analysis of some aspects of criminal careers in a rapidly changing environment of transition from authoritarian regime to democracy and market economy.
pp.179-186